Planetary Health Starts at Home: Why North Carolina Must Act Now
The views expressed in this post are those of the author and not necessarily of CACHE leadership and its members.
“Remember who you came from.”
I have carried these words with me for years—across conference halls, disciplines, and the spaces where public health tries to make sense of complex systems. Lately, I have been thinking about them again while watching the conversation around climate and health unfold here in North Carolina.[1]
Climate change is often framed at a distance: melting ice sheets, global temperature curves, projections for the year 2100. Yet in North Carolina, the story is already intimate. It is present in patients with heat exhaustion, in clinics, schools, and businesses navigating storm-related disruptions, in the farmworker moving through another dangerously hot summer day. The question is no longer whether climate change will affect health here...it already is.
The language of planetary health helps name what many of us in public health have been observing in fragments. At its core is a simple recognition: the conditions that support human health are inseparable from the stability of Earth’s natural systems. When those systems destabilize, health risks follow (Figure 1).
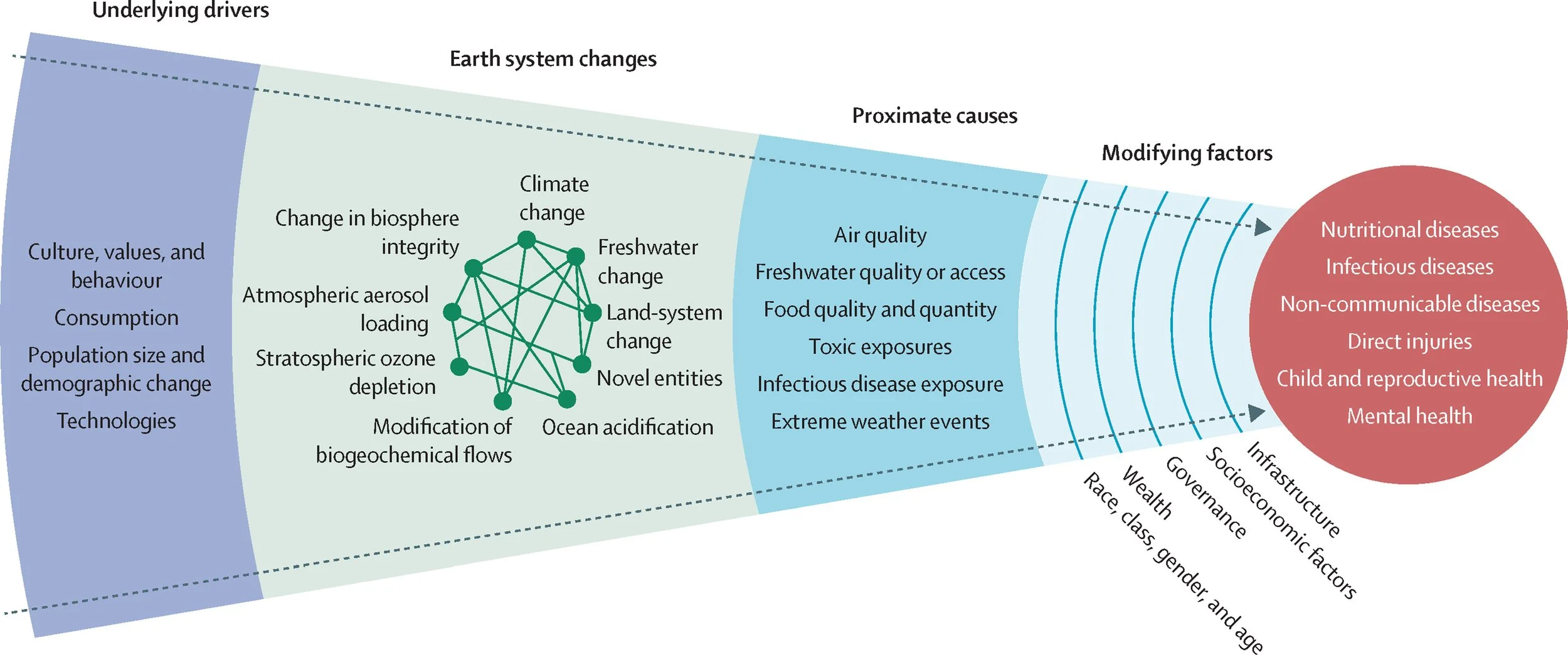
Figure 1. Schematic illustrating the framework of planetary health (from Myers et al 2025, The Lancet, https://doi.org/10.1016/S0140-6736(25)01256-5)
Recent data suggests that six of nine planetary boundaries that regulate the Earth system have already been transgressed. But the more important point, at least from where I sit, is this: health harms do not wait politely for thresholds to be crossed. They emerge earlier, unevenly, and often along familiar fault lines of inequity.
In North Carolina, those fault lines are visible.
Farmworkers—many of whom are essential to the state’s agricultural economy—are working through intensifying heat and degraded air quality. Low-wealth communities and communities of color (especially African American, Indigenous, and Latinx/Hispanic communities) continue to face disproportionate risks from flooding, hurricanes, wildfires, and extreme heat. Rural health systems are asked to maintain continuity of care even as extreme weather events grow more frequent and disruptive. These are not abstract projections. They are lived realities unfolding in real time.
The planetary health framework insists on something else that feels deeply resonant with public health practice: justice is not marginal—it is central. The burdens of climate change fall most heavily on populations who have contributed least to the problem. In North Carolina, we see this pattern repeat itself across geography, occupation, and race. Thus, any serious response to climate and health must grapple not only with emissions and infrastructure, but with equity, power, and protection for those most at risk.
Across the state, health professionals are beginning to organize around this reality.
Carolina Advocates for Climate, Health, and Equity (CACHE) brings together physicians, nurses, public health practitioners, and allied health professionals who share a growing concern: climate change is already straining both population health and health care delivery in North Carolina.
CACHE’s vision—that all North Carolinians, especially those most at risk, can achieve health and wellbeing in the face of a changing climate—feels both ambitious and vital. Its work reflects an understanding that the health sector sits in a complicated position: we are responders to climate-related illness, but we are also contributors to the emissions and pollution that worsen health disparities.
This is where climate-smart health care becomes more than a buzzword or lofty goal. Reducing health care emissions, strengthening resilience to extreme weather, advancing health equity, and leading sustainable transformation in health systems are not siloed targets. They are mutually reinforcing pathways toward protecting the most disenfranchised communities in a disruptive climate.
Still, health system reforms alone will not be sufficient. Planetary health literature increasingly calls for a “health in all policies” approach—an idea that resonates strongly in a state like North Carolina, where climate risks intersect with labor policy, energy systems, housing, and transportation.
What might this look like in practice?
It could mean stronger, enforceable heat protections for outdoor workers, including farmworkers. It could mean investing in climate-resilient hospitals and clinics, particularly in rural and historically under-resourced areas. It could mean accelerating the transition to clean energy in ways that simultaneously reduce emissions and the air pollution that drives asthma, cardiovascular disease, and premature death. It could mean ensuring that clinicians are trained to recognize and manage climate-related illness—because many were not taught to do so.
Importantly, these actions produce immediate and local health benefits.
Cleaner energy improves respiratory and cardiovascular health. Safer working conditions reduce heat-related illness. More resilient infrastructure protects continuity of care when disasters strike. When we more fully account for the true health costs of environmental degradation—and the health benefits of prevention—climate action begins to look less like a distant environmental agenda and more like core public health practice.
North Carolina has the pillars needed to lead in this space: academic institutions, engaged health systems, community-based organizations with deep local knowledge, and a growing network of climate-informed health professionals. But progress cannot be achieved by relying on these aspects alone and requires sustained attention and commitment, cross-sector collaboration, and a willingness to act with urgency.
For those of us working at the intersection of climate and health, the task ahead may feel daunting.
The planetary health framework reminds us that the health of our communities and ecosystems are not separate conversations.
They are one conversation, unfolding across different scales. If we are serious about protecting health in North Carolina, we must also be serious about stabilizing the systems that make health possible in the first place. That means centering equity. It means listening to and partnering with the communities most affected. It means using the trusted voice of the health sector to support evidence-based, justice-oriented climate policy.
And perhaps, in the spirit of those words that have stayed with me—remembering who we came from—it means grounding our work in care: for people, for place, and for the planetary systems that sustain us all.
Because in the end, planetary health is not only a global concept. It is already here, in North Carolina, asking what we will choose to do next.
[1] North Carolina rests on ancestral homelands of many tribal communities. I recognize and honor the Indigenous peoples for whom these were ancestral lands as well as all Indigenous people who live and work in the region today. For more information, please visit this link.